Concept
The concept of stress and autonomic dysfunction
The term “stress” has several meanings and definitions. However, the theory proposed by McEwen (McEwen, Gianaros 2011) has been generally accepted (see Figure 1): Stress involves a stressor and a stress response. The imminent or perceived stimulus that initiates the stress response is called the stressor. The stress response is controlled by the autonomic nervous system.
The brain works consciously and unconsciously. The unconscious brain, the autonomic nervous system, works 24 hours a day. It organizes all bodily functions as well as all conscious behavior related to these functions, including any physical, mental, emotional, psychological, or social behavior.
The unconscious brain varies in activity between being relaxed and being tense like a mechanical spring: it is relaxed when we sleep and tense when we anticipate or are met with a challenge or a threat.
When the work of the brain is in balance, the shift between being relaxed and being tense happens within seconds when needed, such as when there is an unexpected event while driving a car. This ability to shift is called brain resilience, and when normal the brain reacts to the challenge with an adaptive and transient stress response that is constructive and increases performance. This is positive stress and is also called transient or acute stress. Afterwards, the relaxed state is re-established by processes of homeostasis aiming at maintaining a constant condition of the internal environment (see Figure 1).
If a person is under a too high stress load for a too long period and with insufficient restitution in between, the balance is lost, and the unconscious brain loses its resilience. This leads to dysfunction of the adaptive transient stress response, a condition called autonomic dysfunction, which is associated with a variety of physical, mental, emotional, psychological, and/or social dysfunctions. This reduces overall performance and may affect health negatively. In this situation, stress has become negative and destructive and is also called persistent or chronic stress (see Figure 1). If the autonomic dysfunction persists, it may lead to diseases such as depression, anxiety, PTSD, hypertension, chronic pain, reduced fertility, diabetes, heart disease, and/or stroke.
There is a close association between the function of the autonomic nervous system, stress, and the PPS (Pressure Pain Sensitivity) measure as the autonomic nervous system is controlling both the stress response and the PPS measurement, and they change in parallel during transient and persistent stress (see Figure 1 and 2).
Persistent stress affects 1/3 of the working population according to a recent EU report. Persistent stress has a bi-directional association to the non-communicable diseases such as diabetes, obesity, and cardiovascular diseases. Presently, these diseases account for 80 % of national health care budgets in Western countries. According to WHO, the prevalence of these diseases will increase during the coming decade.
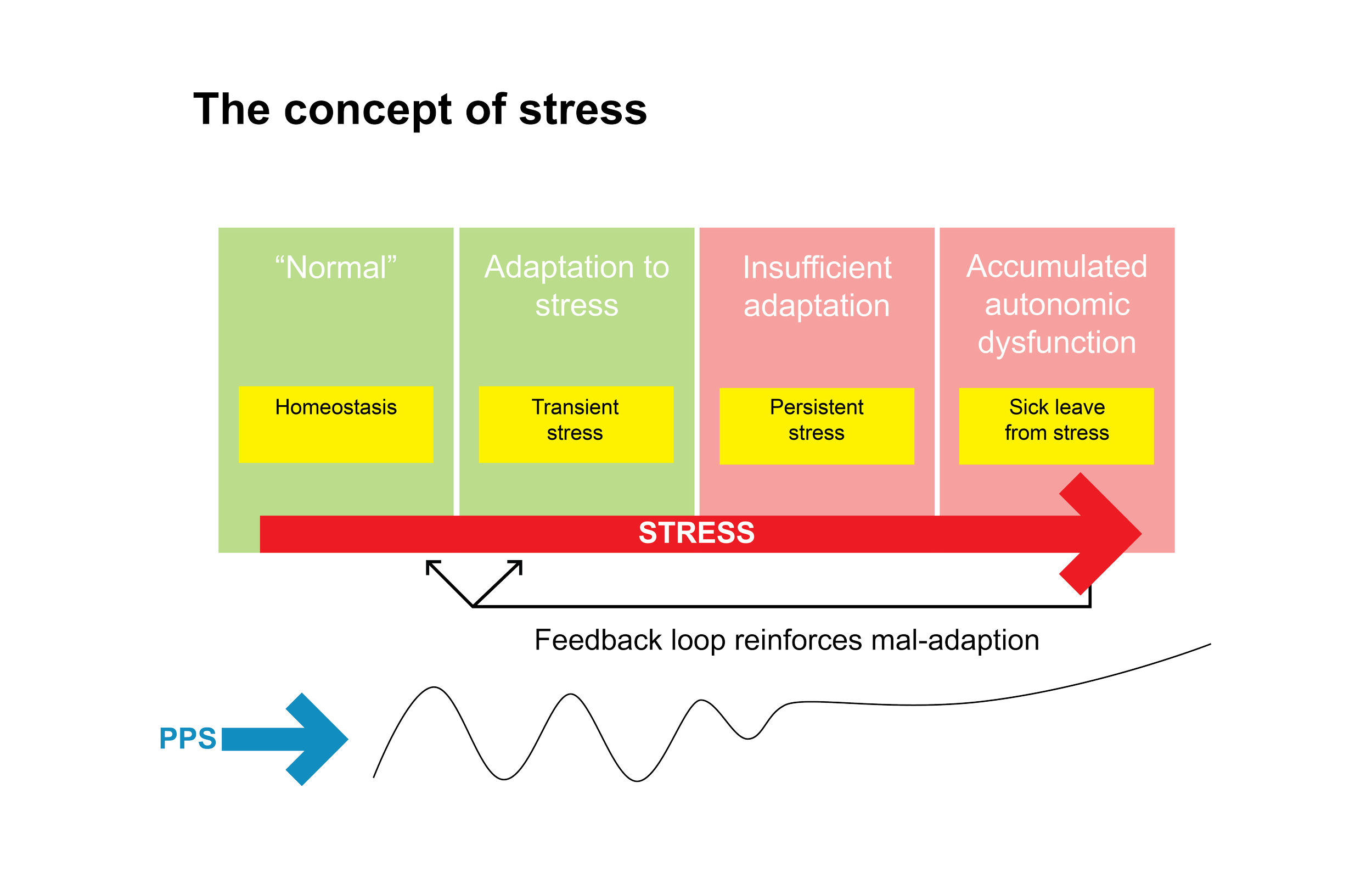
Figure 1: The concept of stress. The green area marks the healthy and constructive transient stress. The body mobilizes resources in an adaptive response to a perceived challenge or threat and returns to the resting state (homeostasis) when the challenge is over. The PPS measurement increases and decreases in parallel with the level of stress. The red area marks the unhealthy destructive state of autonomic dysfunction and persistent stress. The adaptive response works inadequately, and the body is in a condition with a persistently elevated level of stress. The PPS measurement is also elevated during rest and thus persistently elevated (after McEwen, Gianaros 2011).

Figure 2: The association between stress, PPS measurement, and autonomic nervous system function. An external or internal stimulus causes the perception of a challenge or threat by the unconscious control center in the brain, which in response activates an adaptive physiological process with a broad bodily impact mediated by the autonomic nervous system, including an elevation of the pressure pain sensitivity of the chest bone (PPS).

Figure 2b: The development of a chronic state of autonomic nervous system dysfunction.

A: normal state; B: transient stress; C persistent stress; D: Daily non-noxioussensory nerve stimulation, see intervention
Figure 2c Periosteal Pressure Sensitivity (PPS) duringacute and persistent stress, and during the non-pharmachological intervention described (daily non-noxious sensory stimulation

